


A resource for reliable information about significant people, places, events, and things in Minnesota history.

Civil War surgical instruments and case, 1861-1865. This kit used by a Fifth Minnesota Infantry Regiment surgeon, with its prominent amputation saws and scarificators for bloodletting, illustrates the reliance of physicians in the era before germ theory on "heroic" medical interventions.
Minnesotans have long considered health to be as central to their identity as the weather; in fact, to recruit settler-colonists, Minnesota's early promoters touted the state's distinctive, supposedly fever-free climate and its potential to foster health. The settler-colonists who responded shaped health in Minnesota in turn, altering the physical environment with their tools and the social environment with their traditions of cooperative self-help.
Thus, a modern public health infrastructure grew side by side with medicine in an expanding state. Innovations in medical care and in models for its delivery developed as responses to local conditions and needs, and became products that could be exported to the nation and the world.
Minnesotans' intimate relationship with the natural environment has been, at times, a double-edged sword: long winters and isolation have strained mental health; agricultural practices have polluted the water and threatened the health of farm communities; sparse population and rural distances have produced disparities in access to medical care. Still, Minnesotans see their state as a healthy place, one in which the production of health and medicine has become big business.
Explorers' accounts of the Minnesota territory do not describe a health paradise. Father Louis Hennepin's 1683 account of his travels with Native Americans records sickness, fatal rattlesnake bites, and chronic hunger.
By the 1780s, new diseases carried by Europeans, notably smallpox, were causing deadly epidemics in the non-immune Native American population. The disease, starvation, and cultural destruction among Native Americans that resulted from interaction with Europeans arguably quickened the decline of the Upper Mississippi Valley fur trade by reducing the ranks of Native hunters.
European-American settler-colonists also suffered epidemics. Steamboats carried cholera up the Mississippi River to St. Paul in 1854 and 1855. St. Paul's newspapers, city council, and city board of health worked together to suppress information about the epidemic, lest it undermine the area's healthful image. The Sisters of the Order of St. Joseph of Carondelet responded more pragmatically, opening the state's first hospital, St. Joseph's, in St. Paul in 1854.
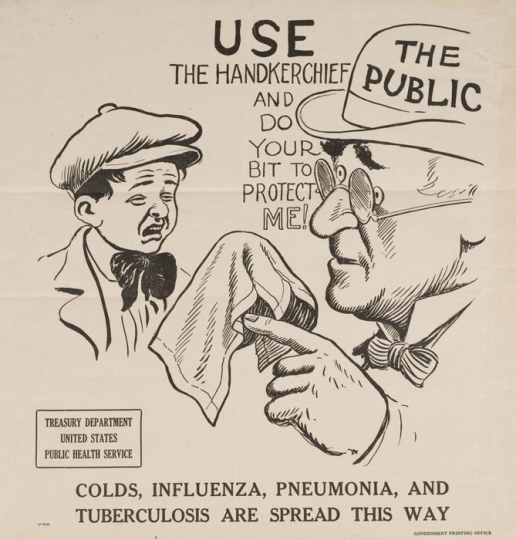
Published guides to Minnesota appealed to invalids—the medical tourists of the nineteenth century. But even as these guides described Minnesota's "fever-free" landscape and its frosty air as a help for lung problems, consumption (tuberculosis) accounted for almost 15 percent of deaths in the state in 1872. In fact, Minnesota mirrored trends elsewhere in the United States from the late 1800s into the early 1900s. Infectious diseases such as measles and scarlet fever were rampant: hundreds of Dakota women, children, and elders died of disease and malnutrition while kept at Fort Snelling after the US–Dakota War; diphtheria and typhoid epidemics were common until the 1910s; and smallpox outbreaks—preventable through vaccination—continued into the 1930s. Medical treatments for these illnesses were limited, and many people relied on midwives, healers, and home remedies rooted in their ethnic traditions rather than physicians.
Ole Edvart Rølvaag's epic novel Giants in the Earth describes the toll that long winters, isolation, backbreaking work, and the grasshopper plagues of the 1870s took on the mental health of settler-colonists. Urbanization and the recruitment of young immigrant workers for Minnesota's new farms, mines, and lumber camps loosened the family and community ties that had traditionally provided care for the mentally ill, disabled, and elderly.
To support the state's expanding social and medical needs, charitable and religious organizations and state government established new institutions. St. Peter State Hospital for the Insane (later renamed St. Peter State Hospital) opened in 1866; by 1900, the state had five public mental institutions.
One challenge for Minnesota leaders was keeping the state's new citizens healthy and productive by preventing disease. In 1872, Minnesota followed Massachusetts and California in establishing a state board of health. Responsibility for public health rested with local communities' part-time health officers and boards of health, while the state board set policy and provided support services.
Minnesota was putting public health structures in place as old humoral and miasmatic theories of disease causation were giving way to germ theory, the idea that specific pathogens cause specific diseases. Germ theory offered compelling logic for new public health measures, such as regulation of the cleanliness of food and water supplies. The State Board of Health provided sanitary inspection services and in 1896 established a bacteriological laboratory, replacing the Secretary of the Board of Health's personal lab, which had been used for water analyses since 1873.
Meanwhile, environmental changes caused by humans drove an increased demand for medicine. Steam laundries, knitting mills, grain mills, and mines produced occupational respiratory diseases. Mechanized agriculture, sawmills, railroads, and industry mangled workers' bodies daily and caused occasional catastrophes, such as the 1878 Washburn flour mill explosion in Minneapolis. The artificial limb companies that were started to serve Civil War amputees thrived with the steady demand from victims of industrialization.
Unlike eastern states, which had hospitals and medical schools dating back to the eighteenth century but were just creating public health departments in the 1880s, Minnesota developed its medical system in tandem with its modern public health infrastructure, in response to the specific needs of the growing state. In 1883, the state legislature passed a law regulating who could practice medicine, and by the end of the 1880s, there were five hospitals in the Twin Cities and several medical colleges.
New medical graduates William and Charles Mayo joined their father's medical practice in Rochester in this period. In an era before residency training, the Mayos became surgical specialists by practicing on a large number of cases and by observing and reading about other surgeons' work. But it was the combination of the Mayos' medical craft, the modern facilities and nursing care provided by the Sisters of St. Francis at St. Mary's Hospital, and an expanding railway network that made Rochester a medical destination. Patients were attracted to the specialized, but integrated, expertise at the Mayo Clinic, which pioneered the efficient management of patients and information within group practice.
Licensing doctors was not enough by itself to elevate the quality of medical practice in Minnesota; in 1888, Minnesota medical leaders sought to improve care by standardizing medical education under the umbrella of the University of Minnesota, the state's land-grant university. By 1909, all the state's small, proprietary medical colleges had merged into the University's College of Medicine. As Minnesota's only medical school, the College of Medicine offered medical students basic science and laboratory experience, and clinical education in its hospital, which also provided care for the state's poor. These attributes earned the college rare praise in the Carnegie Foundation's 1909 survey of American medical schools. Two years later, Minnesota became the first medical school in the nation to require a year of hospital experience (internship) for the MD degree.
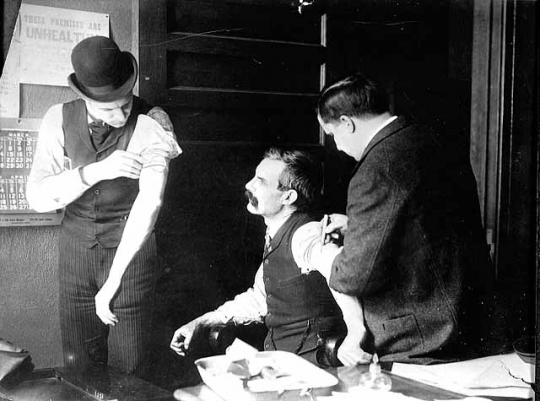
While Rochester and the Twin Cities were becoming regional medical centers focused on individual health, the state health department was taking on population health threats. This was sometimes contentious: on the grounds of individual rights or potential negative commercial impacts, individuals and business interests opposed measures such as mandatory smallpox vaccination and restrictions on travel and public gatherings during the influenza epidemic of 1918. Minneapolis could not agree on milk pasteurization until 1948. The Minnesota Sanatorium for Consumptives at Ah-Gwah-Ching opened in 1907, the first of a network of state and county hospitals where people with active tuberculosis were preventatively isolated and treated. However, many tuberculosis sufferers resisted being sent to these hospitals.
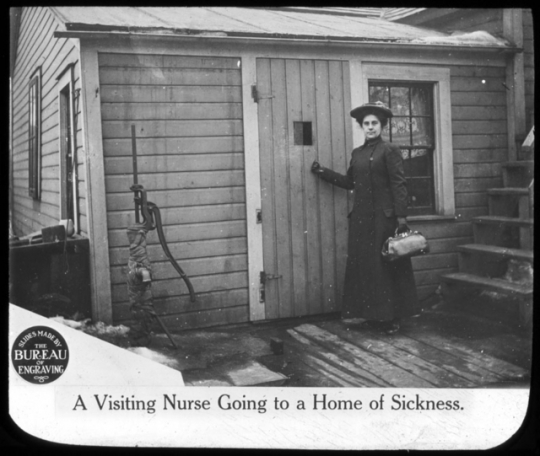
By the 1910s, the state's attention shifted from attracting new settler-colonists and controlling infectious disease to breeding healthy citizens and preventing chronic disease. Federal funds encouraged the state health department to establish a Division of Child Hygiene in 1922. The division targeted high infant mortality, employing public health nurses to provide prenatal and well-baby care in rural areas and poor urban neighborhoods, and on Native reservations. The focus on cultivating a healthy future population took a coercive form, however, in the state's 1925 eugenics law. In the decades that followed the law's passing, more than 2,200 so-called defective residents at the School for the Feeble-Minded in Faribault, Minnesota, were surgically sterilized.
Across the twentieth century, support for public health in Minnesota has been paradoxical: the state has benefited from an activist Board of Health and progressive social welfare programs, both public and private, but going back to the 1920s, its per capita spending on public health has lagged behind some of the poorest states in the country.
Still, by most measures, health status for white Minnesotans has consistently ranked among the best in the nation since at least 1945. Higher incomes and educational levels probably have played a role, as have the state's prosperity and commitment to the common good. All of these factors have contributed to a higher proportion of citizens with health insurance at the turn of the twenty-first century than the national average.
As Minnesota emerged from the Depression and World War II, its economy was increasingly shaped by its medical enterprises. These enterprises also influenced medical science and practice throughout the world, as they exported medical knowledge, technology, and skilled practitioners. Mayo Clinic chemist Edward Kendall isolated the hormone that led to the development of cortisone, for which he shared the 1950 Nobel Prize in Physiology or Medicine. Australian nurse Sister Elizabeth Kenny received a rare positive reception among the faculty at the University of Minnesota Medical School in 1940 for her physical therapeutic approach to polio. The Sister Kenny Institute in Minneapolis brought polio patients, physicians, and research money to Minnesota; by the mid-1940s, Kenny's method had overtaken traditional immobilizing therapies for polio.
The University of Minnesota nurtured innovation and research in this period. Physiologist Ancel Keys's work on nutrition became common knowledge—he invented the "K-ration" for soldiers in World War II as well as the "Mediterranean diet," based on his Seven-Country Study of diet and cardiovascular health, which continues to inform contemporary medicine. Owen Wangensteen established the University's surgery department as an international center for research and training; pioneer transplant surgeons Norman Shumway and Christiaan Barnard earned PhDs there.
The simple, disposable bubble oxygenator that helped transform heart surgery was developed by Richard DeWall and C. Walton Lillehei at the University. They used it for their frequent operations on newborns with blue-baby syndrome—cyanotic heart defects caused by nitrates from fertilizers leaching into wells and groundwater, linked to Minnesota's agricultural environment.
Engineer Earl Bakken and Medtronic, the small company he founded in his garage in 1949, supported University surgeons' technical needs and, in the process, launched Minnesota's medical device industry. More than sixty years later, the state's biobusiness technology sector encompasses hundreds of firms employing more than 34,000 people, with revenues of more than $11 billion in 2007.
Minnesota's dominant food and agricultural industries have had sometimes contradictory consequences for global and state health. Nutritional-deficiency diseases like pellagra were made worse in the late nineteenth century by Minnesota companies' adoption of new degerming and milling technologies; but in the 1940s, nutrition science and food industry processes added nutrients back into the flour and baked goods Minnesota supplied the world. University of Minnesota agronomist Norman Borlaug won the 1970 Peace Prize for his contributions to the Green Revolution—engineering high-yield crops to feed the world's expanding population. However, the chemically intensive farming methods of the Green Revolution era created new health problems in the form of water pollution and increased rates of cancer for agricultural workers and rural residents.
Minnesota remained a mostly rural state three decades longer than the nation as a whole. Until 1950, half of the state's population lived in rural areas or in towns of 2,500 or less. However, changes in the countryside, the rise of hospitals and medical technology, and reliance on medical insurance to pay for care favored the health of city-dwellers. Poorer access to medical care in rural areas was more evident than ever by the end of the 1930s, and federal and state efforts to improve it helped only a little. The federal Emergency Maternity and Infant Care Act for low-ranking soldiers' families in World War II increased the percentage of Minnesota babies born in hospitals, and the 1946 Hill-Burton Hospital Construction Act helped fund new hospitals in 29 Minnesota communities in its first four years alone.
Medicine has been a profitable state industry, but Minnesotans' geographic and financial access to care has been an increasing issue since World War II. Racial disparities in disease incidence, mortality, and life expectancy also have revealed an unhealthy underside to the state's reputation for social equality. To address the problem of access, Community Health Associates in Two Harbors (1944) and Group Health Plan in the Twin Cities (1957) built on the state's historic tradition of cooperatives to offer prepaid direct medical service plans to members. Innovative models for the organization and delivery of care—group practice; cooperative health plans; the 1973 law requiring that health maintenance organizations (HMOs) be nonprofit; public health insurance for children; and the 1992 MinnesotaCare insurance plan for low-income citizens—have reflected a distinctly Minnesota approach and have provided leadership for the nation.
By the 1970s, pride in Minnesota's natural environment was tinged with concerns about health risks, such as Lyme disease and mercury-contaminated fish. Human actions had altered the state's landscape, and environmental hazards could no longer be easily hidden.
Legislative and judicial initiatives sought to address existing hazards, just as the State Board of Health had policed hygienic perils seven decades earlier. Citizens' organizations and state and federal governments sued Reserve Mining Company for dumping taconite tailings with asbestos-like fibers into Lake Superior and polluting municipal water supplies along the North Shore. But the damage has been long-lasting: today, Northern Minnesota residents and miners exhibit excess rates of mesothelioma, a rare lung cancer caused by asbestos exposure.
In 1975, Minnesotans tackled chronic disease by becoming the first state to prohibit smoking in restaurants and other public places. The state also was among the first to sue the tobacco industry successfully, arguing that cigarettes caused multiple health problems in the population, thus raising the costs of public health and medical health care for thousands of patients in state-funded insurance programs.
Minnesota has a critical stake in national debates about universal health coverage, the education and distribution of the medical workforce, climate change and environmental policies, and the responsibility of government for the health and well-being of its citizens. Following national trends, health care and medicine will likely remain cornerstones of the state's economy, but new people, new needs, and new attitudes will shape Minnesota's health status in the context of the twenty-first century.
Jennifer Gunn is an associate professor and Director of the Program in the History of Medicine at the University of Minnesota. She is the author of Plains Practice: A History of Rural Health and Medicine in the Upper Midwest, 1900-1950.

Benoit, Virgil. "Gentilly: A French-Canadian Community in the Minnesota Red River Valley. Minnesota History 44, no. 8 (Winter 1975): 278–289.
http://collections.mnhs.org/MNHistoryMagazine/articles/44/v44i08p278-289.pdf
Blegen, Theodore C. Minnesota: A History of the State. St. Paul: Minnesota Historical Society Press, 1963.
Bollet, A.J. "Politics and Pellagra: The Epidemic of Pellagra in the U.S. in the Early Twentieth Century." Yale Journal of Biology and Medicine 65 (1992): 211–221.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2589605/pdf/yjbm00051-0058.pdf
Bulletin of the History of Medicine 84 (2010): 323–357.
"Child Rearing Hazards Reduced," Minnesota's Health 3 (1949): 1.
Clapesattle, Helen. The Doctors Mayo. Minneapolis: University of Minnesota Press, 1941.
———. "Health and Medicine in Rochester, 1855–70." Minnesota History 20, no. 3 (September 1939): 221–242.
http://collections.mnhs.org/MNHistoryMagazine/articles/20/v20i03p221-242.pdf
———. "When Minnesota Was Florida's Rival." Minnesota History 35, no. 5 (March 1957): 214–221.
http://collections.mnhs.org/MNHistoryMagazine/articles/35/v35i05p214-221.pdf
Creevy, C.D., and M.M. Weaver. "Requirement of Internship for Graduation." Academic Medicine 20 (1945): 216–225.
Dublin, Louis I. "48 States of Health." The American Magazine 140 (1945): 34–35+.
Faribault State School and Hospital Records. Minnesota Historical Society and Minnesota State Archives. St. Paul, Minnesota.
"Medicine: The Fat of the Land." Time Magazine, January 13, 1961.
Folsom, William Henry Carman. E.E. Edwards, ed. Fifty Years in the Northwest. With an introduction and appendix containing reminiscences, incidents, and notes.
St. Paul: Pioneer Press Company, 1888.
Freedman, Ben. "The First State Public Health Laboratories in the United States." Public Health Reports 69 (1954): 867–875.
Fye, W. Bruce. "The Origins and Evolution of the Mayo Clinic from 1864 to 1939: A Minnesota Family Practice Becomes an International 'Medical Mecca.' " Bulletin of the History of Medicine 84 (2010): 323–357.
Gilman, Rhoda. "Last Days of the Upper Mississippi Fur Trade." Minnesota History 42, no. 4 (Winter 1970): 122–140.
http://collections.mnhs.org/MNHistoryMagazine/articles/42/v42i04p122-140.pdf
Grady, Denise, "Slaughterhouse 12," New York Times, February 5, 2008. Late Edition (East Coast).
Haines, Michael. "Fertility and Mortality in the United States." EH.net Encyclopedia. http://eh.net/encyclopedia/fertility-and-mortality-in-the-united-states/
Hartley, E.C., and Ruth E. Boynton. "A Survey of the Midwife Situation in Minnesota." Minnesota Medicine 7 (1924): 439–446.
Harwick, Harry J. Forty-Four Years with the Mayo Clinic: 1908-1952. Rochester, Minnesota: Harry J. Harwick, 1957.
Hennepin, Father Louis. "Narrative of the Voyage to the Upper Mississippi from his 'Description de la Louisiane,' printed at Paris, in 1693." In Discovery and Exploration of the Mississippi Valley, with the Original Narratives of Marquette, Allouez, Membré, Hennepin, and Anastase Douay. John Gilmary Shea, ed. New York: Redfield, 1853.
"Hennepin, Louis." Dictionary of Canadian Biography Online.
http://www.biographi.ca/en/bio.php?BioId=34963
Hill-Burton Hospital Grant Program. History of Medicine Division. National Library of Medicine. Bethesda, Maryland.
Huffman, Thomas R. "Exploring the Legacy of Reserve Mining: What Does the Longest Environmental Trial in History Tell Us About the Meaning of American Environmentalism?" Journal of Policy History 12 (2000): 339–368.
Jordan, Phillip D. The People's Health: A History of Public Health in Minnesota to 1948. St. Paul: Minnesota Historical Society, 1953.
Kaplan, Anne, and Marilyn Ziebarth. Making Minnesota Territory, 1849-1858. St. Paul: Minnesota Historical Society Press, 1999.
Kaups, Matti. "A Finnish Savusauna in Minnesota." Minnesota History 45, no. 1 (Spring 1976): 11–20.
http://collections.mnhs.org/MNHistoryMagazine/articles/45/v45i01p011-020.pdf
Ladd-Taylor, Molly. "Coping with a 'Public Menace': Eugenic Sterilization in Minnesota." Minnesota History 59, no. 6 (Summer 2005): 237–248.
http://collections.mnhs.org/MNHistoryMagazine/articles/59/v59i06p237-248.pdf
Lass, William E. "Minnesota: An American Siberia?" Minnesota History 49, no. 4 (Winter 1984): 149–155.
http://collections.mnhs.org/MNHistoryMagazine/articles/49/v49i04p149-155.pdf
Lillehei, C. Walton. "Chapter 1: Historical Development of Cardiopulmonary Bypass in Minnesota." In Cardiopulmonary Bypass: Principles and Practice, 2nd edition. Glenn P. Gravlee, Richard F. Davis, Mark Kursz, and Joe R. Utley, eds. Philadelphia: Lippincott Williams and Wilkins, 2000.
Meier, Peg. Bring Warm Clothes: Letters and Photos from Minnesota's Past. Minneapolis: Minneapolis Tribune, 1981.
Miles, Steven H., Nicole Lurie, Lois Quam, and Arthur Kaplan. "Health Care Reform in Minnesota," New England Journal of Medicine 327 (1992): 1092–1095.
Minnesota Agency History Records. Minnesota Historical Society and Minnesota State Archives. St. Paul, Minnesota.
Minnesota Department of Health. "Four new cases of asbestos-related cancer to be included in University of Minnesota's Taconite Workers Health Study." Press release, March 30, 2010.
http://taconiteworkers.umn.edu/news/pages/Four%20new%20cases%20of%20asbestos-related%20cancer%20to%20be%20included.html
Minnesota Department of Health Records. Minnesota Historical Society and Minnesota State Archives. St. Paul, Minnesota.
Najarian, John S., and J. Michael Cecka. "Norman E. Shumway, MD, PhD (1923–2006)." Clinical Transplantation 20 (2006): 269–271.
Norton, Jeffrey A. "History of Endocrine Surgery." In Surgery: Basic Science and Clinical Evidence, 2nd edition. Jeffrey A. Norton, Philip S. Barie, R. Randal Bollinger, Alfred E. Chang, Stephen F. Lowry, Sean J. Mulvihill, Harvey I. Pass, and Robert W. Thompson, eds. New York, New York: Springer, 2008.
O'Keefe, Michael. "Social Services: Minnesota as Innovator." Daedalus 29 (2000): 247–267.
Phelps, David, "After 10 years, smoke clears on state's tobacco lawsuit." Minneapolis Star Tribune, January 26, 2008.
Qualey, Carlton C. "A New El Dorado: Guides to Minnesota, 1850s-1880s." Minnesota History 42, no. 6 (Summer 1971): 215–224.
http://collections.mnhs.org/MNHistoryMagazine/articles/42/v42i06p215-224.pdf
Rajakumar, K. "Pellagra in the United States: A Historical Perspective." Southern Medical Journal 93 (2000): 272–277.
The Robins, Kaplan, Miller, and Ciresi, LLP, website. Minnesota Tobacco Litigation.
http://www.robinskaplan.com/verdicts-and-settlements/mn-tobacco-litigation
Rogers, Naomi. " 'Silence Has Its Own Stories': Elizabeth Kenny, Polio, and the Culture of Medicine." Social History of Medicine 21 (2008): 145–161.
Rølvaag, Ole E. Giants in the Earth: A Saga of the Prairie. Translated from the Norwegian by Lincoln Colcord and the author. New York: Harper & Brothers, 1927.
The United Health Foundation website. America's Health Rankings. Minnesota (2010).
Uphoff, Mary Jo, Walter H. Uphoff, and Russell Lewis. Group Health, an American Success Story in Prepaid Health Care. Minneapolis: Dillon Press, 1980.
Wall, Barbra Mann. Unlikely Entrepreneurs: Catholic Sisters and the Hospital Marketplace, 1865–1925. Columbus: Ohio University Press, 2005.
Weiner, Lynn. " 'Who Are Wanted in Minnesota.' " Labor History 18 (1977): 403–406.
Wikipedia. Tobacco Master Settlement Agreement.
http://en.wikipedia.org/wiki/Tobacco_Master_Settlement_Agreement
Wilder, R.M. "A Brief History of the Enrichment of Bread and Flour." JAMA (1956) 162: 1539–1541.
Willoughby, Kelvin. "Minnesota's Competitive Position in the Biobusiness Technology Industries—Executive Summary." Minneapolis: The BioBusiness Alliance of Minnesota, 2011.
Wilson, Leonard G. Medical Revolution in Minnesota: A History of the University of Minnesota Medical School. St. Paul: Midewiwin Press, 1989.
Wolf, Jacqueline H. " 'Let Us Have More Mother-Fed Babies': Early Twentieth-Century Breastfeeding Campaigns in Chicago and Minneapolis." Journal of Human Lactation 15 (1999): 101–105.
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
The health and identities of Minnesotans have been shaped by their intimate relationship with the natural environment, for good and for ill.
The state's early promoters treated the distinctive climate and its potential to foster health as marketable assets to recruit settler-colonists.
Early settler-colonists shaped health in Minnesota by bringing diseases that killed many non-immune Native Americans, and by altering the physical environment with their tools and the social environment with their cultural traditions of cooperative self-help.
Unlike older states that had established medical institutions first, in Minnesota, a modern, activist public health organization grew side by side with the medical infrastructure.
Innovations in medical care and in models for its delivery developed as responses to local conditions and needs, and became products that could be exported to the nation and the world.
The production of health and medicine has developed into big business for Minnesota, with the Mayo Clinic and the medical device industry as significant examples.
White Minnesotans have enjoyed among the highest life expectancy and health status in the nation, linked to higher incomes and educational levels, and progressive social welfare policies that have resulted in higher proportions of residents being covered by health insurance.
Over time, there has been an increasing gap between rural and urban access to health care, and growing racial disparities in disease incidence, mortality, and life expectancy.
Minnesota has contributed to national and global health through its training of health and medical personnel, provision of medical services, medical innovations, and its contributions to nutrition and agricultural sciences.
The Sisters of the Order of St. Joseph of Carondelet open St. Joseph's Hospital, the first hospital in the state, and nurse victims of the cholera epidemic that had traveled up the Mississippi River on steamboats to St. Paul.
The Minnesota State Board of Health is established. It goes on to provide progressive state and national leadership in public health.
St. Mary's Hospital opens in Rochester, providing a modern facility for the surgical practice of William Worrall Mayo and his two sons, Charles and William, and supporting the development of the Mayo Clinic.
All of the medical schools in the state merge into the University of Minnesota's College of Medicine, an arrangement that makes Minnesota a model of medical education reform.
An influenza pandemic occurs, killing more than 10,000 Minnesotans; World War I ends and many rural communities with unspent Red Cross funds contribute them to hire county public health nurses.
With federal matching funds from the Sheppard-Towner Maternity and Infancy Protection Act of 1921, the Minnesota Department of Health establishes a Division of Child Hygiene to reduce infant and maternal mortality in the state.
Australian nurse Sister Elizabeth Kenny presents her physical therapeutic methods for the treatment of polio to the faculty of the University of Minnesota's medical school, which begins to teach the Kenny Method.
The Hill-Burton Hospital Survey and Construction Act passes, providing federal funds for new hospitals and health centers, especially in rural areas; by 1950, more than 29 communities in Minnesota are approved for new hospitals.
Medtronic is founded. It builds upon the surgical innovations of C. Walt Lillehei, Richard DeWall, and others at the University of Minnesota in the 1950s to create pacemakers and medical devices.
To protect the public's health from environmental hazards, new laws and court cases tackle air and water pollution in the state. These include a lawsuit against Reserve Mining Company and the 1975 Clean Indoor Air Act.
The MinnesotaCare Act is passed. It provides a sliding-scale medical insurance program for the uninsured and exemplifies Minnesota national leadership and innovation in the organization of and payment for medical care delivery.
Made possible by the Arts and Cultural Heritage Fund through the vote of Minnesotans on November 4, 2008. Administered by the Minnesota Historical Society.
Minnesota Historical Society • 345 W. Kellogg Blvd., St. Paul, MN 55102-1906 (Map) • 651-259-3000 © MNHS.
Send questions or comments to mnopedia![]() mnhs [dot] org. View our Privacy Policy.
mnhs [dot] org. View our Privacy Policy.






Great article on the history
Great article on the history of health and medicine in Minnesota. One question from the bibliography section: the Bruce Frye article cited there includes the title of the article, but not the journal, volume, date, etc., where it was published. Could that be added?